
Progressive Supranuclear Palsy (PSP) is a rare neurodegenerative disorder that primarily affects movement, balance, speech, swallowing, vision, mood, and cognition. Although PSP is relatively rare, with a prevalence of 5.8 to 6.5 per 100,000 people, it is considered the most common atypical form of Parkinsonism. The incidence increases with age, particularly after 60, and the average age of onset is around 65 years.
How does PSP occur?
The exact cause of PSP remains unclear, but age is the most significant risk factor. Some studies suggest that environmental factors, such as toxins used in agriculture, and genetic predispositions, particularly variants in the MAPT gene, may increase the risk of developing the disease. PSP is characterized by abnormal accumulation of hyperphosphorylated tau protein in neurons, particularly in brain regions controlling movement, balance, cognition, and vision. This leads to widespread neuronal death and dysfunction, disrupting normal neurological functions.
Common Symptoms of PSP:
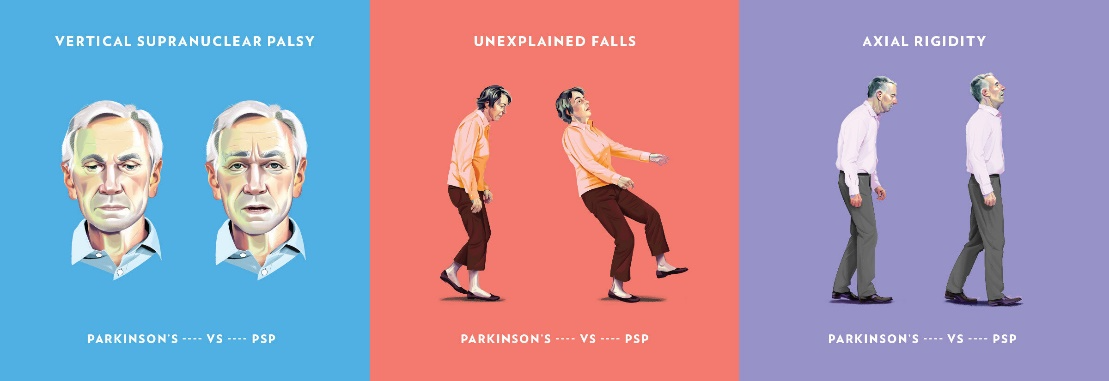
The symptoms of PSP are progressive and affect both motor and non-motor functions. The most prominent motor symptoms include postural instability, frequent backward falls, bradykinesia, axial rigidity, and dystonia. PSP patients typically adopt a stiff, upright posture, in contrast to Parkinson’s disease (PD) patients, who lean forward. Vertical gaze palsy, particularly downward gaze difficulty, is a hallmark of PSP, contributing to falls and impairing activities like reading and eating. Involuntary eye movements, known as square wave jerks, and blepharospasm (uncontrolled blinking) are also common.
Speech and swallowing difficulties (dysarthria and dysphagia) often appear early and worsen over time, leading to communication challenges and an increased risk of aspiration pneumonia. Cognitive symptoms in PSP include executive dysfunction, apathy, and impulsivity. Patients may struggle with planning, multitasking, and making decisions. Emotional incontinence, such as inappropriate laughing or crying, is also observed. It is worth noting that PSP is often confused with Parkinson’s disease due to overlapping symptoms like bradykinesia and rigidity. However, several features distinguish PSP from PD. PSP patients typically present with early vertical gaze palsy, axial rigidity, and faster disease progression. In contrast, PD patients have more pronounced limb involvement and respond well to dopaminergic medications like Levodopa, while PSP patients show minimal response to such treatments.
How is this condition managed?
There is no cure for PSP, and treatment is mainly focused on managing symptoms of this condition. Dopaminergic medications like Levodopa may offer temporary relief for rigidity and bradykinesia in some patients, but most do not experience significant improvement. Other medications, such as Amantadine and SSRIs, may provide modest benefits for motor and mood symptoms. Botulinum toxin injections can help manage dystonia and blepharospasm. Other therapies used to manage PSP include physiotherapy and exercise, speech therapy and occupational therapy. With this in mind, exercise has shown to be the most beneficial conservative treatment in managing the symptoms of this condition and maintaining overall quality of life.
How does exercise help?
Exercise is crucial in managing PSP, as it helps maintain mobility, balance, and overall function. Balance training, gait training, and strength exercises are key components of therapy. Gait retraining and oculomotor exercises may also provide benefits in improving movement coordination and visual adaptation. Though evidence supporting specific exercises for PSP is limited, regular physical activity has been shown to delay the progression of disability and improve quality of life. Some benefits of exercise include:
Benefits of Exercise in PSP:
- Improved Balance and Fall Prevention:
- Balance training reduces the risk of falls, which are a leading cause of injury in PSP patients.
- Strength and Mobility:
- Resistance training helps counteract muscle weakness, which contributes to gait disturbances and postural instability.
- Cardiovascular Health:
- Aerobic exercise, such as walking or cycling, maintains cardiovascular fitness and promotes overall well-being.
- Mental Health and Cognitive Function:
- Exercise has been shown to improve mood and reduce anxiety and depression, which are common in PSP. There is also evidence suggesting that regular exercise can help slow cognitive decline.
- Increased Flexibility: Regular stretching and flexibility exercises prevent joint stiffness, which is exacerbated by axial rigidity